TED is a lifelong, progressive, debilitating autoimmune disease distinct from Graves’ disease
IGF-1R activation on orbital fibroblasts is a cause of the progression1
IGF-1R activation on orbital fibroblasts is a cause of the progression1
IGF-1R ACTIVATION ON ORBITAL FIBROBLASTS
CAUSES INFLAMMATION AND EXPANSION OF MUSCLE AND FAT TISSUE BEHIND THE EYE
that can result in a wide range of visible and nonvisible signs and symptoms and significantly impact a patient’s daily activities and quality of life1-4
THE UNDERSTANDING OF TED HAS EVOLVED1,5
It was once thought that TED could only be treated non-surgically when the disease was considered "active" or "acute"—the only time it impacts patients’ quality of life
We now know that, as an autoimmune disease, TED has a negative impact on patients’ lives throughout the course of the disease and thus can be treated non-surgically at any point
AS WITH OTHER AUTOIMMUNE CONDITIONS, TED PATIENTS CAN EXPERIENCE FLARES, LEADING TO PERIODS OF INCREASED INFLAMMATION AND OTHER DISEASE MANIFESTATIONS6-8
Thyroid eye disease, or TED, is a serious, progressive, and debilitating autoimmune disease.
Emerging research demonstrates that the orbital fibroblast, a specialized cell responsible for tissue repair, is central to the pathophysiology of TED.
Pathogenic orbital fibroblasts are believed to recruit fibrocytes and lymphocytes that infiltrate the orbit.
Fibrocytes differentiate into orbital fibroblasts, which enhance T-cell proliferation and activation.
T-cells and B-cells activate orbital fibroblasts and secrete cytokines, thyroid-stimulating hormone receptor, or TSHR, autoantibodies, and insulin-like growth factor-1 receptor, or IGF-1R, autoantibodies, which contribute to the inflammatory cascade.
Two co-localized receptors reside on the surface of orbital fibroblasts:
TSHR and IGF-1R, a gatekeeper of orbital fibroblast activation.
Autoantibodies activate TSHR and IGF-1R, and cross talk mediated by beta-arrestin creates a receptor-signaling complex that stimulates orbital fibroblasts.
INFLAMMATORY CASCADE AND POTENTIAL CONSEQUENCES OF TED
Once activated, orbital fibroblasts proliferate and produce inflammatory cytokines and hydrophilic hyaluronan, which enlarges orbital tissue volume.
Activated orbital fibroblasts differentiate into adipocytes and myofibroblasts, which contribute, respectively, to adipogenesis and fibrosis of the orbital tissues.
The ensuing tissue expansion and remodeling leads to crowding in the fixed bony orbit, and this may have long-term sequelae.
Damage and Consequences can include: Proptosis, Diplopia, Strabismus, Eyelid retraction, Erythema, Excessive tearing, Chemosis and in rare, extreme cases Corneal ulceration, optic nerve compression, and optic neuropathy, or blindness.
Cross talk between TSHR and IGF-1R, as well as IGF-1R-mediated immune function, may play a critical role in the pathophysiology of TED.
Understanding the cross talk may be vital to addressing this debilitating disease.

TARGETING IGF-1R ACTIVATION MAY HELP
REDUCE INFLAMMATION AND PREVENT MUSCLE AND FAT TISSUE REMODELING, AS WELL AS EXPANSION BEHIND THE EYE.1
While MRI imaging is not required to diagnose TED, it can provide objective confirmation of the substantial inflammatory changes in and around the orbit and show the involvement of individual muscles9
Some TED patients may initially experience nonvisible symptoms like eye pain and blurry vision4,12
IN A STUDY OF PATIENTS DIAGNOSED WITH BOTH TED AND GRAVES’ DISEASE 71% (N=17) OF UNTREATED GRAVES' DISEASE PATIENTS WITH NO VISIBLE SIGNS OF TED SHOWED EXTRAOCULAR MUSCULAR SWELLING IN ORBITAL MRI10
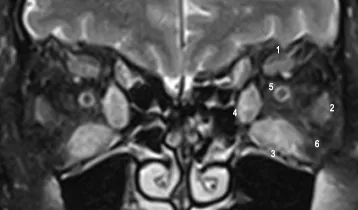
Normal MRI13
Case courtesy of Mohd Radhwan Bin Abidin,
Radiopaedia.org, rID: 155793
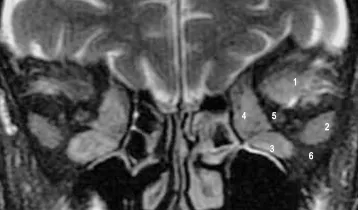
MRI with findings suggestive of moderate TED14
Case courtesy of Qutaiba Jaf'ar Mahmoud,
Radiopaedia.org, rID: 167879
Coronal T2 fat saturation MRI showing moderate enlargement and inflammation/edema of the superior (1), lateral (2), inferior (3), and medial (4) recti muscles and orbital fat (6) bilaterally. The optic nerve (5) appears normal.*
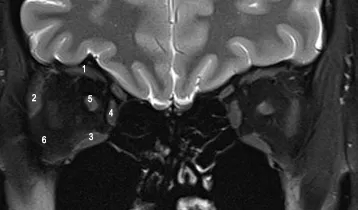
MRI with findings suggestive of severe TED15
Case courtesy of Roberto Schubert,
Radiopaedia.org, rID: 13874
Coronal T2 fat saturation MRI showing severe enlargement and inflammation/edema of the superior (1), lateral (2), inferior (3), and medial (4) recti muscles and orbital fat (6) bilaterally. There is also minimal crowding of the left optic nerve (5).*
*The numbers correspond with the numbers in the images above.
Up to 90% of TED patients have a thyroid condition18
TED has been referred to as Graves’ orbitopathy (GO), Graves’ ophthalmopathy, thyroid-associated orbitopathy (TAO), Graves’ Eye Disease, or thyroid ophthalmopathy3
In Graves’ disease, TSHR autoantibodies drive inflammation of the thyroid epithelial cell membranes11; in TED, IGF-1R autoantibodies activate and cause inflammation of the orbital fibroblasts, which can lead to a range of clinical symptoms1-3
The connection between TED and other thyroid conditions highlights the importance of screening all patients with a thyroid condition who are experiencing ocular signs and symptoms of TED19

TREATING ONLY THE THYROID GLAND WON’T TREAT TED1-3,11
IGF-1R, insulin-like growth factor-1 receptor; MRI, magnetic resonance imaging; TSHR, thyroid-stimulating hormone receptor; T2, transverse relaxation time.
Receive the latest news and updates about Thyroid Eye Disease (TED).